Understanding standards for face masks and respirators
Guidance for manufacturers of medical or surgical face masks and respirators on the standards and key performance aspects required for inclusion in the Australian Register of Therapeutic Goods (ARTG).
Purpose
The TGA is currently undertaking a post-market review of face masks included in the Australian Register of Therapeutic Goods (ARTG).
The TGA is aware there are many different standards available to manufacturers; and we are familiar with differences between these standards.
The TGA has also identified common areas of non-compliance against claimed standards throughout this review process.
This Guidance intends to assist manufacturers in choosing appropriate standards and to set out the TGA's expectations for performance testing of respirators, surgical respirators and medical/surgical facemasks, before inclusion in the ARTG.
The information provided may be useful to manufacturers and sponsors, as well as health care facilities and health care personnel.
This information is not exhaustive and not designed to be a checklist for compliance with the Essential Principles.
This guidance will be updated periodically to provide further clarity for both manufacturers and sponsors.
More information on regulation of PPE and different types of masks and respirators is provided at Regulation of Personal Protective Equipment and COVID-19.
A summary of some of this information is available in a guidance video on face masks:
Background
Face masks meet the definition of a medical device when the following claims are made:
- the face mask is to be used for the prevention of the transmission of disease between people, or
- the face mask is suitable for therapeutic use such as for surgical, clinical, medical use, or use in other health services.
If the manufacturer's labelling, advertising, or documentation contain the claims above, the face mask is considered to be a medical device and is required to be included in the ARTG.
All classes of medical devices need Conformity Assessment evidence before they can be manufactured and supplied.
Conformity Assessment is the systematic and ongoing examination of evidence and procedures to ensure that a medical device (including IVD medical devices) complies with the Essential Principles.
These Principles relate to safety and performance aspects of the device including its design and construction.
Demonstrating compliance with them establishes that the product is safe and fit for its intended purpose.
The manufacturer should maintain an active and robust quality management system (QMS) and the application of sound manufacturing practices for evaluating risk and in the design and construction of medical devices.
The intended purpose needs to suitable for the device and it must perform in the way intended by the manufacturer. (See Annex 1 for table of appropriate GMDN codes for masks and respirators and Face masks and respirators that are regulated by the TGA for further TGA advice on regulation of face masks).
Manufacturers of all medical devices (including IVD medical devices) manufactured and/or supplied in Australia should ensure they have:
- appropriate conformity assessment procedures in place for the device
- appropriate documentation demonstrating compliance of the device with the Essential Principles.
Compliance with the Essential Principles can be demonstrated by showing that your product meets an applicable standard.
Note
Although the use of standards to demonstrate compliance with the Essential Principles is not mandated under the Regulations, the TGA recognises certain standards to assist manufacturers in complying with the conformity assessment procedures and the Essential Principles.
Standards
A range of standards may be of assistance to manufacturers of respirators surgical respirators and medical/surgical masks, including:
- standards that can be applied broadly for any medical device
- standards related to performance specifications of certain types of devices/products
- standards, sub-parts of standards and published procedures related to the application of a specific test methods to evaluate specific performance criteria.
When choosing which standards to apply to each device, manufacturers should take into consideration the:
- intended purpose of the device
- environment in which it is likely to be used
- likely users of the device
- generally acknowledged state-of-the-art; or the level of development reached at any particular time usually as a result of modern methods.
Table 1 below identifies a non-exhaustive list of standards that may be considered by the manufacturers when determining how to minimise risk associated with the device and demonstrate compliance with the conformity assessment procedures and the Essential Principles.
A device should only claim compliance with a standard if it meets all the applicable clauses based on the device design and the intended purpose.
Table 1 highlights certain standard clauses that are of particular importance for respirators and surgical/medical face masks to effectively prevent disease transmission in a medical setting.
The listed performance parameters have also been identified as common causes of non-compliance in regulatory surveillance.
For Australian manufacturers, NATA accredited laboratories may provide testing services to evaluate your product against the referenced standard clauses.
Again, these performance aspects are non-exhaustive, and evidence needs to be provided to support any additional performance claims.
Note
It is preferable that any evidence submitted, be from a laboratory holding accreditation from NATA (or equivalent accreditation issued by an ILAC certified body) for the test(s) applied.
If evidence from a non-accredited laboratory is submitted, this may not be considered acceptable evidence, unless other information can be provided to support the reliability of the analysis (e.g. SOPs, method validation and raw data from the testing laboratory for the tests applied).
In some cases, we may require you to provide specific technical details in relation to how testing has been conducted to support any test reports or certificates submitted (including from an accredited laboratory).
Technical information required may include (but is not limited to) the:
- standard operating procedures (SOPs)
- work-instructions
- testing worksheets/records
- photographs of the samples tested
- method validation reports
- calibration records, or
- details of equipment used by the test laboratory.
| Product type | Typical intended purpose(s) | Important performance parameters | Standards, sub-parts of standards, procedures and requirements |
|---|---|---|---|
| Any Medical Device | Quality Management Systems | Systems to demonstrate an organisation's ability to provide medical devices and related services that consistently meet customer and applicable regulatory requirements. | ISO 13485:2016 ISO 9001:2015 |
| Any Medical Device | Application of risk management | Processes for a manufacturer to identify the hazards associated with a medical device to estimate and evaluate the associated risks, to control these risks, and to monitor the effectiveness of the controls. | ISO 14971:2019 |
| All Medical Devices | Labelling | Sufficient and accurate information to be provided with the medical device | Therapeutic Goods (Medical Devices) Regulations 2002 - Schedule 1 - Section 13 - Information to be provided with medical devices |
| Devices in Contact with Skin | Biocompatibility | Biological Evaluation of Medical Devices and testing within a risk management framework. | ISO10993-1:2018 |
| Tests for in vitro cytotoxicity, designed to determine the biological response of mammalian cells in vitro to a device and or extracts of a device. | ISO 10993-5:2009 | ||
| Assessment of medical devices and their constituent materials with regard to their potential to produce irritation and skin sensitisation. | ISO 10993-10:2010 | ||
| Surgical/Medical Face Mask | Requirements for single use medical masks intended to provide barrier protection between the mouth and nose of the wearer and immediate environment | General requirements and classifications | AS 4381:2015 EN 14683:2019 ASTM F2100-20 YY 0469-2011 |
| Fluid resistance | ISO 22609:2004 ASTM F1862/F1862M-17 | ||
| Bacterial filtration efficiency | ASTM F2101-19 EN 14683:2019 Annex B | ||
| Breathability | EN 14683:2019 Annex C | ||
| Respirator | Requirements for respirators intended to provide protection against airborne particles | General requirements and classifications | AS/NZS 1716:2012 (P2/P3 classes) 42 CFR 84 (N-, R- and P- classification at 95, 99 and 99.9% filter efficiency) EN 149:2001 + A1:2009 (FFP2/FFP3 classes) GB2626:2019 (KN and KP 95/100 classes) |
| Particulate filtration efficiency | AS/NZS 1716:2012 Appendix I NIOSH TEB-APR-STP-0059 (N95) EN 13274-7:2019 | ||
| Breathability | AS/NZS 1716:2012 Appendix G NIOSH TEB-APR-STP-0003 NIOSH TEB-APR-STP-0007 EN 149:2001 + A1:2009 Clause 8.9 GB 2626:2019 Clause 6.5 and 6.6 | ||
| Fit (Leakage) | AS/NZS 1716:2012 Appendix D EN 149:2001 + A1:2009 Clause 8.5 GB 2626:2019 Clause 6.4 | ||
| Head strap and head harness | The breaking strength of each head strap shall be at least 10 N. | ||
| Surgical Respirator/Medical Protective Mask | Requirements for surgical respirators intended to provide protection against airborne particles and fluid resistance | Surgical respirators should comply with performance requirements of relevant respirator standards and also demonstrate the appropriate level of fluid resistance like surgical masks. | GB 19083:2010 AS/NZS 1716:2012 42 CFR 84 EN 149:2001 + A1:2009 GB2626:2019 ISO 22609:2004 ASTM F1862/F1862M-17 https://www.standards.org.au/news/new-guidance-for...https://www.standards.org.au/news/new-guidance-for-respiratory-protective-equipment-released Exhalation valve is not acceptable in surgical respirators due to unfiltered exhaled air. |
Note
Standards Australia is adopting ISO 16900 to transition away from AS/NZS 1716:2012.
Manufacturers are encouraged to keep informed of changes to relevant standards.
Typically, application of a currently adopted standard is considered a minimum benchmark for applying solutions having regard to the generally acknowledged state of the art.
Application of superseded standards is generally not acceptable.
Manufacturers should consider how they will transition standards as they change and consider risk management activities such as a gap analysis to understand any potential impacts.
Application of testing methods
When considering application of testing methods to assess the performance of medical devices, there are a number of elements manufacturers should consider in order to determine what methods should be applied, and how they should be applied.
This typically includes:
- the intended purpose of the device
- the design of the device, taking into consideration
- materials, construction, and manufacturing processes
- if different parts of the device relate to different functions that contribute to achieving the intended purpose
- the results of any design calculations, risk analysis, investigations, technical tests, or any other tests carried out in relation to the device
- post-market monitoring of the device.
Sampling plans
A systematic and periodic testing schedule is essential in ensuring consistent and adequate product quality of medical devices.
A proper sampling plan is critical to ensure the sample results are reflective of the quality of the device group which the samples are drawn from.
The sampling plan is a combination of the sample size and the acceptability criteria. It should be determined based on appropriate risk assessments and sound statistical methods.
Testing should be an ongoing part of the manufacturer’s technical documentation and triggered as specified by the manufacturer’s quality management procedures, such as when changes are made to the design, product specifications, production methods, suppliers or raw materials of the product.
Some of the respirator and medical mask standards prescribe the sampling plan or the sample size requirements for specific tests.
However, it should be recognised that:
- there are noted differences between the sampling requirements of different standards for similar tests
- it may not be adequate to test to the selected standards without understanding the context of the sampling plan or without appropriate risk assessments
- it may be insufficient to only present test results of isolated, limited lots, especially without demonstration of adequate quality management systems.
For medical/surgical facemasks, we expect manufacturers to make available test evidence of conformity for fluid resistance, bacterial filtration efficiency and breathability:
- to the acceptable quality limit (AQL) of 4.0% and the general inspection level II
- on 3 non-consecutive lots or justification to demonstrate that lot to lot variability in performance is acceptable.
An AQL of 4.0% is referenced by multiple relevant standards, including ASTM F2100-20, ISO 22609:2004, and ASTM F1862/F1862M-17.
Examples of acceptable sampling plans can be found in ISO 2859-1:1999 or ASQ/ANSI Z1.4. Sampling plans should be established with consideration to the inspection level, lot size and AQL and known manufacturing tolerances and quality.
We recommend general inspection level II unless otherwise statistically justified.
Note
Specifically for fluid resistance, both ISO22609:2004 and ASTM F1862/F1862M-17 require:
- at minimum 32 samples to be tested per test
- masks to meet an AQL of 4%.
The TGA requires both these conditions to be met, that is a minimum of 32 masks tested per batch, and each batch tested to be accepted by a sampling plan to AQL 4%, General Inspection level II (or a plan providing comparable Consumer Risk Quality levels as described below), dependant on your batch size and manufacturing quality output.
This means that for lot sizes greater than 280, a sample size greater than 32 is required to demonstrate an AQL 4.0% at General Inspection Level II, Normal Inspection.
The YY 0469:2011 and EN 14683:2019 (optionally) require a sampling size of 3-5 units depending on the tests applied.
Such limited sample size is deemed insufficient to demonstrate safety, consistency and quality of the device and therefore not recommended.
When formulating a sampling plan, it is impossible to achieve all three options of minimising the sample size, minimising the consumer risk (failure to detect a performance issue) and minimising producer risk (rejecting acceptable product lot).
For a large lot size, a single sampling plan to the AQL of 4%, General Inspection Level II, requires a considerable amount of samples to be tested.
To reduce the burden of large testing regimes while still ensuring sufficient consumer protection, manufactures may consult the operating characteristic (OC) curves in the ISO 2859-1:1999 and derive appropriate sampling plans which achieve an acceptable risk to the consumer comparable to the AQL of 4%, General Inspection level II.
Such customised sampling plans may require smaller sample size but incur higher risk to the producer.
It is a trade-off that the manufacturers can choose between.
Figure 1: Key performance aspects for medical or surgical face masks and respirators
{kind=link}
A diagram in the shape of a triangle to demonstrate the key performance aspects for medical or surgical face masks and respirators:
- sample size (top)
- consumer risk (left)
- producer risk (right).
ISO 2859-1:1999 is designed for continuing series of lots, under a controlled manufacturing process which should account for switching rules.
Thus, the manufacturers should apply relevant tests to successive lots and switch between normal/tightened/reduced inspections based on the results.
To demonstrate performance specifications are maintained across production lots.
Example of AQL OC Curve Implementation
A manufacturer is producing batches of surgical masks greater than 35,000 and wants to test fluid resistance to an AQL of 4%, General Inspection Level II, Normal Inspection.
The appropriate single sampling plan defined in ISO 2859-1 or ASQ Z1.4 requires 315 items to be tested with a Pass/Fail criteria of 21/22.
A Consumer Risk Quality (CRQ) of 8.84% is derived from this sampling plan (10% batch acceptance).
The manufacturer decides that they want to reduce the requirement for testing fluid resistance on every batch and decides to incorporate alternate samples methodologies that will lower the batch testing requirements, whilst ensuring that the equivalent CRQ remains the same or less.
Below is a table of some of the sampling plans that may be available to a manufacturer in this scenario, noting that if a batch fails testing, then it will not be released.
| Sampling plan type | Sampling plan | Consumer risk quality | Sample size | Pass/fail criteria |
|---|---|---|---|---|
| Single | AQL 4%, Code M | 8.84% | 315 | 21/22 |
| AQL 1,5%, Code J | 8.16% | 80 | 3/4 | |
| AQL 0.4%, Code G | 6.94% | 32 | 0/1 | |
| AQL 1%, Code H | 7.56% | 50 | 1/2 | |
| Double | AQL 4%, Code M | 8.84% | 200/200 | 9/14--23/24 |
| AQL 1%, Code H | 5.94% | 32/32 | 0/2--1/2 | |
| Multiple | AQL 1%, Code H | 5.85% | 26/13/13/13 | 0/2--0/2--0/2--0/2--1/2 |
Respirator standards typically either do not specify sampling requirements or have not provided justifications for the sample size chosen.
For respirators and surgical respirators devices, the TGA requires manufacturers to provide test evidence of conformity on three non-consecutive lots.
For the PFE test, the number of samples tested must be at least 10 or the sample size requirement of the referenced standard (Table 2), whichever is larger.
| Standards (common designation) | AS/NZS 1716:2012 (P2) | 42 CFR 84 (N95) | EN 149:2001+A1:2009 (FFP2) | GB 2626:2019 (KN95) | GB 2626:2006 (KN95) | GB 19083: 2010 |
|---|---|---|---|---|---|---|
| PFE testing sample size by the Standard | Unspecified | 20 | 9 | 20 | 15 | 6 |
Manufacturers are encouraged to formulate the sampling plans for respirator related tests based on appropriate statistical methods, such as by consulting the OC curves in the ISO 2859-1:1999.
The AQL should be determined based on risk assessments but is recommended to be 4% or better given the AQL requirement for medical/surgical facemasks.
Any customised sample plan should also not be in conflict with the requirements in the referenced standards.
TGA requirements for fluid resistance testing
Fluid droplets generated by coughing, sneezing or some medical procedures are widely acknowledged to be a source of pathogen transmission, including the COVID-19 virus1,2,3.
To effectively prevent disease transmission through fluid droplets, face masks must include a fluid resistant barrier.
Fluid resistance will aid in preventing large droplets and splashes from reaching the mouth or nose, potentially transmitting the virus or other infectious agents.
For this reason, we require face masks intended to be used in medical or surgical settings to be resistant to fluid penetration.
For masks regulated as medical devices that claim (or it is implied) to provide fluid resistance, including surgical respirators, the manufacturer should:
- Identify all areas of the mask that are intended to provide a barrier to fluid penetration in the technical documentation for the device. Areas near or covering the mouth and nose must provide a barrier to fluid penetration.
- Hold evidence that the device provides resistance to fluid penetration across all areas of the mask intended to do so.
Attention should be paid to areas of the mask where the material type or thickness differs from the main body material, and any seams located in the central area of the mask covering the nose and mouth.
Note
Not all respirators require compliance with fluid resistance requirements, only surgical respirators.
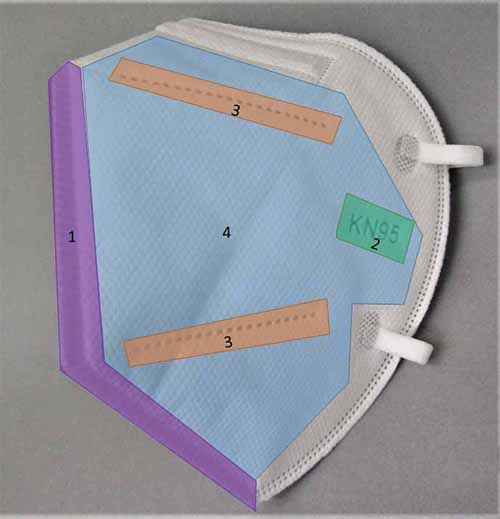
Surgical respirator with 4 identified areas of difference that must be tested for fluid resistance.
{kind=link}
A surgical respirator with 4 identified areas of difference to demonstrate areas that must be tested for fluid resistance:
- a central seam (1, purple)
- embossed KN95 label (2, green)
- embossed lines (3, orange) that are within the central area of the mask covering the nose and mouth
- the main body material (4, blue).
For example, in Figure 2, this surgical respirator has a central seam (1, purple), embossed KN95 label (2, green) and embossed lines (3, orange) that are within the central area of the mask covering the nose and mouth.
All 3 of these areas, in addition to the main body material (4, blue), would need to be tested for fluid resistance level.
Figure 3: Main body (green) of the surgical/medical facemask must be tested for fluid resistance; the perimeter region (red) can be excluded from the testing

{kind=link}
A surgical/medical facemask with areas highlighted in red or green to show which must be tested for fluid resistance (centre, green) and which can be excluded from the testing (the perimeter region (red, perimeter).
For surgical/medical facemasks (Figure 3), the main body (green) is the functionally critical region and needs to be tested for fluid resistance level.
The main body is considered uniform in terms of the structure and the material and therefore is required to be tested once.
Where there are areas of differing material type or thickness in the main body, such as logos, these also need be tested separately.
The perimeter region (red) may be excluded from the fluid resistance testing.
Where standards such as ISO 22609 or ASTM F1862/FM1862M are being used to demonstrate compliance with the Essential Principles, we would expect testing reports to include:
- identification of all areas of the mask that were tested for fluid resistance
- information related to sample pre-treatment and testing methodology conducted by the testing laboratory
- selected blood pressures, volumes, and velocities of synthetic blood used
- the number of samples tested and numbers of pass/ failed samples
- information about the sampling plan used at each location
- any deviations from the requirements of the standard.
We expect all areas of difference will be tested to at a minimum an AQL of 4.0%, General Inspection II.
Each area challenged needs to meet the AQL requirement individually.
TGA Requirements for Sub-micron Particulate Filtration Efficiency (PFE)
Single Use Respirators are disposable devices made from multiple layers of non-woven polymers. They are expected to form a tight seal to a wearer's face.
They are intended to protect the wearer from the transfer of microorganisms and airborne particulate materials while maintaining adequate breathability and comfort.
Respirators are labelled with an effective particulate filtration efficiency for which they have been tested, to ensure they remove the minimum specified percentage of solid and/or liquid aerosols.
Particulate filtration efficiency testing assesses the ability of the mask to protect against infectious agents.
It measures the ability of a respirator to filter out sub-micron sized, electrostatically neutral salt crystals from a stream of air penetrating the mask.
Depending on the nominated standard, the expected filtration efficiency is to be greater than 95%.
The particle sizes are to be sub-micron in line with the respirator's intended purpose, for example filtering bacteria, viruses, and aerosol particulates.
Face masks not regulated by the TGA
Face masks intended for use by the general public for non-medical purposes are not medical devices.
Masks that are not medical devices are not regulated by the TGA.
Examples of such masks include those intended to be used in construction and other industrial applications.
Due to the lack of resistance to fluid penetration, masks designed to certain standards or subclasses of some standards (listed below), may not be suitable for use in medical or surgical settings.
- Type I, II of EN 14683:2019
- YYT 0969:2013
- GB/T 32610-2016
- T/CTCA 1-2019
- T/CTCA 7-2019.
Masks designed and manufactured to comply only with these standards are not suitable for use as a medical device.
These types of masks are not required to be, and should not be, included in the Australian Register of Therapeutic Goods (ARTG).
A suitable standard for reusable masks to demonstrate some of the applicable minimum requirements is ASTM F3502-21.
The standard still specifies the masks are not medical devices but provide further guidelines for manufacturers for this kind of mask.
These masks may still be appropriate for use in non-medical/healthcare settings to assist in reducing airborne disease transmission, along with social distancing measures.
Note
The use of antimicrobial materials, finishes or mechanisms, including that of novel materials, nanomaterials and coatings may be subject to further regulatory scrutiny in consideration of safety and efficacy, as well as potential toxic and adverse effects when these materials or particulates are in contact with skin or is at risk of being inhaled or ingested by the user.
Manufacturer should carefully consider the advertising claims used to not incorrectly advertise products as medical devices.
For more see Face masks and respirators that are regulated by the TGA.
Post-market monitoring and corrective actions
Manufacturers are required to establish and keep up to date a post-market monitoring, reporting and corrective action system.
Where a manufacturer becomes aware of a potential performance or safety issue related to their product(s), the issue should be risked assessed as part of their post-market monitoring and corrective actions systems.
Ideally, through application of policies and procedures defined in a quality management and the application of risk management in accordance with ISO 14971.
For example, if non-compliance with a relevant performance requirement is identified through application of testing methods, the manufacturer should consider the relevance of that information in the context of the intended purpose of the device, and the potential risk the non-compliance presents to the end users.
Following appropriate investigation and evaluation the manufacturer should determine what further action should be taken to:
- Mitigate any immediate unacceptable risk to users;
- This could be through notification of issues and associated risks to users, non-supply or varied supply of stock on hand, or recall of product etc.
- Eliminate or minimise the risk associated with the device in the future
- This could be through appropriate changes the design or production of the device, or variations to the intended purpose etc.
Annex 1: GMDN (Global Medical Device Nomenclature) codes and descriptions
| GMDN | Descriptions |
|---|---|
35177 Mask, surgical, single use | A disposable device made from fabric or other material placed over the nose and mouth by medical personnel to prevent the transmission of airborne organisms while surgery is being performed. |
57793 Public Respirator, single use | A form-shaped filtering mask designed to be placed over the nose and mouth of a member of the general public to permit normal breathing while protecting the wearer from large particles (e.g., blood, body fluids, and airborne particulate materials) and small particles (e.g., bacteria and viruses) when considered necessary (e.g., viral epidemic). It is typically made of multiple layers of non-woven polymers to produce a soft, flexible mask that will create an airtight seal against the user's face and typically secured using elastic head straps or ties; it may incorporate a forming nosepiece (metal wire) and/or an exhalation valve. This is a single-use device. |
57794 Surgical respirator, single use | A non-sterile filtering mask designed to be placed over the nose and mouth of a healthcare worker to permit normal breathing while protecting the worker and patients from the transfer of microorganisms, blood, body fluids, and airborne particulate materials during medical, surgical, dental, and isolation procedures. It is typically made of multiple layers of non-woven polymers, and incorporates a forming nosepiece (metal wire); it is typically secured using elastic head straps. This is a single-use device. |
57792 Antimicrobial surgical respirator | A non-sterile filtering mask designed to be placed over the nose and mouth of a healthcare worker to permit normal breathing while protecting the worker and patients from the transfer of microorganisms, blood, body fluids, and airborne particulate materials during medical, surgical, dental, and isolation procedures; it includes an antimicrobial/antiviral agent to destroy specified pathogens under specified contact conditions. It is typically made of multiple layers of non-woven polymers, and incorporates a forming nosepiece (metal wire); it is typically secured using elastic head straps. This is a single-use device. |
64822 Public face mask, reusable | A flexible, loose-fitting mask designed to be placed over the mouth and/or nose of a member of the general public to permit normal breathing while protecting the wearer from the transfer of large particles (e.g., blood, body fluids, and airborne particulate materials) from the environment, it is not a form-shaped filtering device (i.e., not a respirator). It is made of a flexible, porous fabric or paper material and is typically secured using elastic head straps or ties; it may incorporate a forming nosepiece (metal wire). This is a reusable device. |
64821 Public face mask, single use | A flexible, loose-fitting mask designed to be placed over the mouth and/or nose of a member of the general public to permit normal breathing while protecting the wearer from the transfer of large particles (e.g., blood, body fluids, and airborne particulate materials) from the environment, it is not a form-shaped filtering device (i.e., not a respirator). It is made of a flexible, porous fabric or paper material and is typically secured using elastic head straps or ties; it may incorporate a forming nosepiece (metal wire). This is a single-use device. |
64963 Half-face respirator body/ filter | A form-shaped respiratory mask with filters intended to be placed over the nose and mouth of a person to permit normal breathing while preventing transfer of large particles (e.g. blood, body fluids, and airborne particulate materials) and small particles (e.g., bacteria and viruses) to and from the wearer (i.e., upon inhalation and exhalation). The mask portion is constructed from pliable synthetic polymer materials designed to create and airtight seal against the user's face, and typically includes ties/ head straps; the filters are typically replaceable. This is a reusable device. |
Page history
Title changed from 'Guidance on medical/surgical face masks and respirator standards - key performance aspects' to 'Understanding standards for face masks and respirators' as part of migration to new 'Guidance' content type:
- Consistent ‘Purpose’ heading.
- ‘Legislation’ section to clearly show which laws the Guidance relates to.
- ‘Page history’ section replaces document version history.
- New page navigation features.
- Updated page summaries.
- Complex images include long descriptions.
- New ‘Save as PDF’ feature.
Additional content on details of lab testing from laboratory to match web version.
Update for readability and information on sampling plans. Clarification of fluid resistance testing expectations for surgical respirators.
Update and insertion of requirements on particulate filtration efficiencies.
Original publication.
Title changed from 'Guidance on medical/surgical face masks and respirator standards - key performance aspects' to 'Understanding standards for face masks and respirators' as part of migration to new 'Guidance' content type:
- Consistent ‘Purpose’ heading.
- ‘Legislation’ section to clearly show which laws the Guidance relates to.
- ‘Page history’ section replaces document version history.
- New page navigation features.
- Updated page summaries.
- Complex images include long descriptions.
- New ‘Save as PDF’ feature.
Additional content on details of lab testing from laboratory to match web version.
Update for readability and information on sampling plans. Clarification of fluid resistance testing expectations for surgical respirators.
Update and insertion of requirements on particulate filtration efficiencies.
Original publication.